
Introduction
As individuals age, they face an increased likelihood of experiencing frailty, stemming from a combination of physical, social, mental, and environmental factors. Complex interventions, particularly those tailored through personalized assessments, have proven effective in supporting older adults to live safely and independently. An ideal tool for such assessments should be comprehensive, covering a wide array of domains; person-centered, prioritizing the individual’s needs; validated and reliable for clinical application; acceptable for both users and healthcare providers across different cultures; and informative for health and social care planning at a broader level.
One such needs assessment tool is the EASY-Care tool, developed through collaborations in the United Kingdom, United States, and Europe. Originating in 1994 with a 31-question format known as ‘EASY’, it has undergone revisions in 1999, 2004, and 2010. The current EASY-Care version comprises a three-part questionnaire with 49 core questions, addressing physical, mental, social, and environmental aspects. It integrates questions from established health measurement scales, including the Medical Outcome Scale Short Form 36, Barthel Index of Activities of Daily Living, and the Duke Older Americans Resources and Services Instrumental Activities of Daily Living (Duke OARS IADL). A dedicated not-for-profit organization in the UK manages and licenses the EASY-Care tool, offering detailed information on its website.
While the development of EASY-Care has been documented in several publications, a systematic analysis of its benefits in supporting comprehensive geriatric assessment for older adults living in the community was lacking. This review aims to address this gap by examining the evidence regarding the validity, reliability, and acceptability of EASY-Care. In this context, ‘acceptability’ is broadly defined to include effectiveness, cross-cultural relevance for practitioners and older people, cost-effectiveness, and practicality. This review focuses on empirical evidence but also includes relevant reviews and commentaries for a complete overview. This systematic review was conducted as part of the SOPRANO (Supporting Older People though Assessing Needs and Outcomes) study, which received ethical approval.
Search Methodology and Selection Criteria
A systematic literature search was performed using ‘EASY-Care’ OR ‘EASYCare’ as keywords in titles or abstracts of articles published in English from January 1994 to May 2014. Databases searched included OVID MEDLINE, OVID EMBASE, CINAHL, Web of Science, Cochrane Library, AGEINFO, ASSIA, The National Research Register (NRR) Archive, NICHSR, and NHS CRD DARE/HTA/EED. Reference lists of included articles were also reviewed to find additional relevant studies. Grey literature databases were searched for unpublished materials. Experts at EASY-Care were also consulted for relevant articles.
Articles were included if they:
- Investigated the reliability, validity, or acceptability of EASY-Care.
- Reported on the implementation of EASY-Care in complex interventions, detailing settings, populations, stakeholders, barriers, or facilitators.
- Involved the use of EASY-Care with older people (50 years and over) in community or primary care settings.
- Were published in English.
Two reviewers screened titles and abstracts for ‘EASY-Care’, and full articles were reviewed against the inclusion criteria. Disagreements were resolved through discussion.
Results Overview
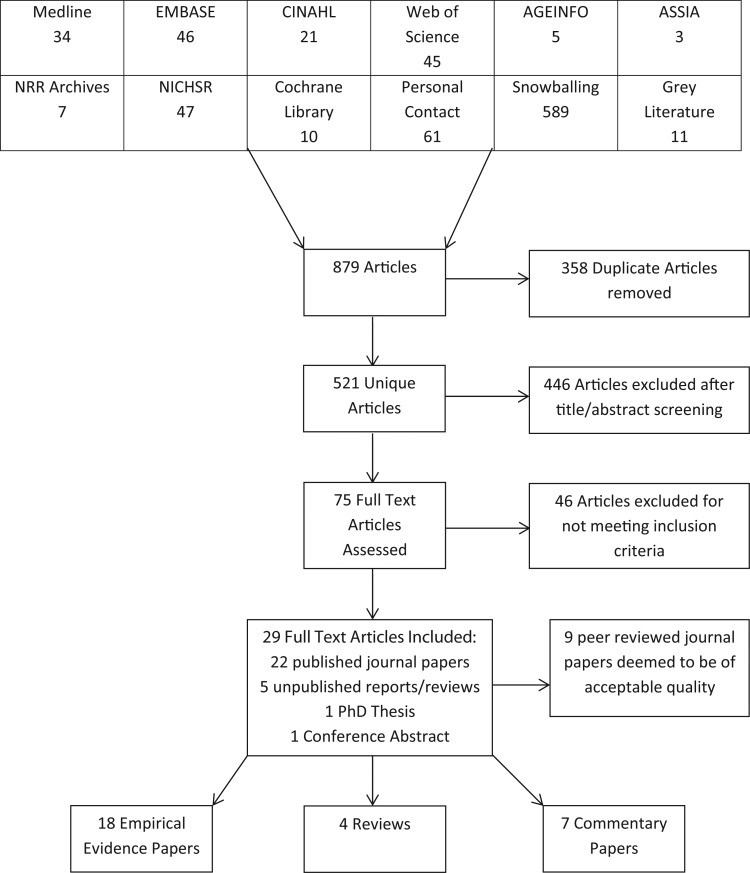
The search yielded 879 articles, with 521 unique articles after removing duplicates (Figure 1). Title and abstract screening excluded 446 articles. The full text of 75 articles was assessed, and 46 were further excluded, resulting in 29 articles included in the review (Table 1).
Figure 1.
 Flow diagram of selected articles included in review
Flow diagram of selected articles included in review
Flow diagram illustrating the article selection process for the review.
Table 1.
Breakdown of included publications by type.
| Publication Type | Authors and Publication Years |
|---|---|
| Empirical Evidence | Bath et al. (2000), Bath et al. (1998), Faculty of Moscow (2008), Fernandes et al. (2009), Jerilu et al. (2013), Keiren et al. (2013), Lambert et al. (2007)a, Lambert et al. (2007)a, Lambert et al. (2009)a, Melis et al. (2008)b, Melis et al. (2008)b, Msambichaka et al. (2014), Philip et al. (2014), Philp et al. (2002), Philp et al. (2001), van Kempen (2013)c, van Kempen et al. (2012)c, van Kempen et al. (2013)c, van Kempen et al. (2014)c |
| Reviews | Foreman et al. (2004), Haywood et al. (2004), Haywood et al. (2005), Martin and Martin (2003) |
| Commentary | Marques et al. (2014), Olde-Rikkert et al. (2013), Philp (1997), Philp et al. (2001), Philp (2000), Richardson (2001) |
Note: a, b, c denote studies with overlapping sample populations.
Fourteen peer-reviewed empirical articles were assessed for quality using CASP checklists. Consensus among reviewers (C.C., N.C., G.S.) identified nine papers of acceptable quality (Table 2). Three papers from one study used EASY-Care in a hospital setting with post-consultant care patients but were included due to the predominantly community-dwelling sample.
Table 2.
Summary of peer-reviewed empirical data of acceptable quality.
| Author | Study Design | Country | Population | Setting | Sample Size | Acceptability | Reliability | Validity |
|---|---|---|---|---|---|---|---|---|
| Keiren et al. | Feasibility study (mixed methods) | Netherlands | Family practitioners, Primary care nurses, Older people | General practice | Professionals = 25, Older people = 9 | ✓ | ||
| Lambert et al. | Cross-sectional study | UK | Older people | Nursing homes, Residential care, hospitals | 119 Older people | ✓ | ||
| Lambert et al. | Cross-sectional study | UK | Older people | Nursing homes, Residential care, hospitals | 119 Older people | ✓ | ||
| Lambert et al. | Cross-sectional study | UK | Older people | Nursing homes, Residential care, hospitals | 119 Older people | ✓ | ✓ | |
| Melis et al. | Randomised control trial | Netherlands | Vulnerable older adults at home | Community | 151 Older people (Intervention = 85, Control = 66) | ✓ | ||
| Melis et al. | Randomised control trial | Netherlands | Vulnerable older adults at home | Community | 151 Older people (Intervention = 85, Control = 66) | ✓ | ||
| Philip et al. | Cross-sectional study (mixed methods) | Colombia, Kerala, Lesotho, UK, Tonga, Iran | Older people, Clinicians | Primary care, Community, Secondary care | Older people = 115, Clinicians = 79 | ✓ | ||
| van Kempen et al. | Qualitative observational study | Netherlands | Frail older adults, family practitioners, PCNs | Primary care | Older people = 161, Professionals = 18 | ✓ | ||
| van Kempen et al. | Validation study | Netherlands | Frail older adults, family practitioners, PCNs | 6 GP practices | 587 older people | ✓ | ✓ | ✓ |
Overview of Included Studies
Table 1 details the types of publications included, spanning empirical studies, narrative reviews, and commentaries on EASY-Care’s development. Empirical studies involved 2,176 older adults (aged 57–99) and 421 practitioners across diverse geographical locations including the UK, Netherlands, Russia, Portugal, Albania, Kosovo, Tanzania, Colombia, Iran, India, and Tonga.
Data Extraction and Synthesis
Data extraction, guided by the CASP tool, focused on study participants, EASY-Care interventions, comparator tools, assessment outcomes, and measures of reliability, validity, and acceptability. Due to the heterogeneity of included articles, a narrative synthesis was conducted instead of meta-analysis, focusing on validity, reliability, and acceptability of EASY-Care.
Validity: Assessing Individual and Population Needs
Validity, the effectiveness of a tool in measuring its intended target, is well-documented for EASY-Care in terms of face, content, criterion, and cross-cultural aspects. However, further research is needed on concurrent and convergent validity. EASY-Care’s validity is partly based on its incorporation of previously validated tools. Geriatric experts contributed to its content, enhancing face and content validity. Comparison against gold standard health measurements in 50 patients showed mixed Cohen’s Kappa values (0.39–1). Good intra-class correlations for loneliness, morale, and disability score supported criterion validity. Linking 63 of 75 Portuguese EASY-Care questions to WHO ICF domains further strengthens content validity. Cross-cultural validation confirms EASY-Care’s international applicability.
Reliability: Consistency in Needs Assessment
Reliability, the consistency of results over repeated administrations, has limited evidence for EASY-Care as a needs assessment tool, with only one article providing data. Test-retest reliability in 50 patients over two weeks showed generally positive kappa values (−0.06 to 0.82). Lower scores in communication, feeding, telephone use, and cognitive impairment were attributed to data spread issues, requiring further testing. Literature up to 2013 cites these figures, indicating a gap in recent reliability assessments for needs assessment or population-level data. Internal consistency data in English publications is absent.
Validity: As a Diagnostic Tool
EASY-Care has also been validated as a clinical decision support tool, EASY-Care Two Step Older Persons Screening method (TOS). Concurrent validity, comparing EASY-Care TOS to Fried Frailty Criteria and Rockwood Frailty Index, showed correlation coefficients of 0.52. Convergent validity against other frailty tools yielded Spearman Rho statistics of 0.458 and 0.573 (both P-values < 0.001). Predictive validity for functional decline and frailty indication was found to be stronger than objective patient measurements, likely due to incorporating GP’s patient knowledge.
Reliability: Consistency in Diagnostic Use
Reliability of EASY-Care TOS was assessed in a small sample (n=19), showing 89% inter-rater agreement and a test–retest kappa value of 0.63, without significant differences. However, the subjective nature of GP decision-making warrants caution regarding EASY-Care TOS reliability.
Acceptability of EASY-Care
EASY-Care is available in paper and electronic formats. Electronic version trials were piloted in the UK in 2004, but results are not yet available. EASY-Care demonstrates high usability in community and residential settings internationally. Both older adults and assessors largely found it feasible, with few reporting difficulties in needs assessment and diagnostic applications. Developers suggest minor re-wording for cultural appropriateness. Assessor feedback is valuable for ongoing development.
Praised for its simple language, EASY-Care is suitable for self-completion or with family assistance, but nurses are considered most suitable for administration. Their interpersonal skills, rapport-building ability, especially with sensitive questions, and capacity to relieve time-constrained GPs are key advantages. Nurses also require less training than volunteers and may offer more objective assessments, addressing potential reporting biases from older adults or carers.
An EASY-Care-based intervention within the Dutch Geriatric Intervention Programme improved patient quality of life cost-effectively, with more successfully treated patients in the intervention group, at a willingness to pay of €34,000.
Discussion
This review indicates strong acceptability of EASY-Care as a personal needs assessment tool, characterized by high feasibility, usability, and some evidence of cost-effectiveness. Validity is supported by inclusion of validated scales, expert geriatrician input, good correlation with other health measures, alignment with WHO ICF classifications, and cross-cultural validity. Reliability evidence is limited, with studies having small samples and data spread issues. Evidence is also limited for EASY-Care’s use in population-level needs assessments and as a frailty diagnostic tool. Practical application evidence is also scarce.
The systematic search provides a robust evidence overview, though the exclusion of non-English articles, including seven in German, French, Dutch, Portuguese, and Polish, may represent a limitation. Despite this, many international studies included reported findings in English, mitigating potential bias.
Given EASY-Care’s accreditation in England’s Single Assessment Procedure (SAP) since 2001, more real-world application evidence was expected. The limited evidence outside research settings prevents definitive conclusions on its practical utility, although it is favored over other accredited tools.
EASY-Care shows promise for care providers globally for community needs assessment and frailty diagnosis. More research on its practical application is needed, building on positive outcomes from the Dutch geriatric intervention program. Results from electronic format acceptability trials would also benefit comprehensive geriatric assessment implementation.
From a commissioning perspective, EASY-Care as a standardized tool can provide population-level data for health and social care planning. Practitioners should consider necessary resources for EASY-Care assessments. In resource-limited settings, EASY-Care can guide efficient resource allocation. Electronic format use could enhance integrated patient information systems, reducing redundant assessments and improving care planning. Considering other needs assessment tools, existing reviews are decade-old, necessitating updated reviews of CGAs.
EASY-Care’s potential benefits align well with nursing practice, both for needs assessment and diagnosis. Its international recognition and consistent participant responses across countries underscore its global applicability. Overall, EASY-Care is a valid, comprehensive, and acceptable tool centered on older adults’ well-being priorities. However, further reliability testing is warranted.
Conclusion
This systematic review offers a comprehensive summary of evidence for the EASY-Care assessment tool across various uses. While validity and acceptability for personal needs assessment are well-supported, reliability evidence and its application for population-level needs assessment or frailty diagnosis are limited. Further research is needed to assess reliability and validity in diverse applications. The limited evidence on this SAP-accredited tool highlights the necessity for studies evaluating EASY-Care’s impact in routine practice.
Key points.
- Reliability evidence for EASY-Care is lacking, requiring further investigation.
- Strong evidence supports the validity and acceptability of EASY-Care for personal needs assessment and its international applicability.
- Evidence suggests that EASY-Care-based interventions can yield positive health outcomes.
Conflicts of interest
None declared.
Funding
This research was funded by the National Institute for Health Research (NIHR) as part of the Collaboration for Leadership in Applied Health Research and Care East Midlands (CLAHRC EM). The views expressed are those of the authors and do not necessarily reflect those of the NHS, NIHR, or the Department of Health.
Supplementary data
Supplementary data mentioned in the text are available online.
Acknowledgements
We thank Dr. René Melis and Judith Long for providing literature.
References
(Selected key references are listed here; the full list is available in supplementary data online).
Associated Data
Supplementary Materials
Supplementary Data (html and docx files available online).